Ch. 1: Focus on Inhalants and Anabolic Steroids
In addition to the kinds of substances we have previously studied that individuals use by inhaling (i.e., by smoking or inhaling vapors), a variety of chemicals intended for medical, cleaning, or industrial uses may be misused by inhaling, as well. Additionally, we need to consider the misuse of anabolic steroids. While these are often used/misused for their effect on body shape and athletic performance, they do have psychoactive effects, as well.
What Is Inhalant Misuse
 Inhalants are volatile substances at room temperature; in other words, they are in a gas, aerosol, or vapor form. Inhalant misuse involves breathing in these substances, inhaling them, in high concentrations. For example, they may be concentrated in plastic bags, in latex/rubber balloons or gloves, or soaked on cloths held over the nose and/or mouth (Baydala et al, 2010). Many (but not all) inhalant substances are legally accessed and easily accessed in the home, workplace, or stores, making their misuse attractive to youth when there are no age restrictions on their purchase or use. Some common terms used to describe inhalant use are sniffing, huffing, and bagging (Baydala et al., 2010; NIDA, 2017a).
Inhalants are volatile substances at room temperature; in other words, they are in a gas, aerosol, or vapor form. Inhalant misuse involves breathing in these substances, inhaling them, in high concentrations. For example, they may be concentrated in plastic bags, in latex/rubber balloons or gloves, or soaked on cloths held over the nose and/or mouth (Baydala et al, 2010). Many (but not all) inhalant substances are legally accessed and easily accessed in the home, workplace, or stores, making their misuse attractive to youth when there are no age restrictions on their purchase or use. Some common terms used to describe inhalant use are sniffing, huffing, and bagging (Baydala et al., 2010; NIDA, 2017a).
Various chemicals included in lists of potentially psychoactive inhalants are (Baydala et al., 2010; NIDA, 2017a):
- nitrous oxide, ether, or chloroform (medical anesthetics, generally not easily accessed legally);
- propane;
- whippets/whipped cream aerosol dispensers;
- nitrites (labeled video head cleaner, room odorizer, leather cleaner, liquid aroma; including amyl nitrites, butyl nitrites called poppers, snappers, amys);
- cleaning fluids, spot remover, degreasers (including benzene);
- gasoline and other fuels or lighter fluid (e.g., butane);
- spray paint, varnish, lacquer, resins;
- paint/lacquer thinner, paint remover, polish remover (including acetone);
- computer keyboard or other electronic contact cleaners;
- felt-tip markers;
- correction fluids (mostly older types);
- glues and adhesive sprays; and,
- other aerosol products, like hair spray, spray deodorant, or vegetable oil sprays.
The psychoactive effects associated with most inhalants are short-lived—a matter of a few minutes. This contributes to a tendency to use the inhalant substance repeatedly over a brief period of time (NIDA, 2017a).
Inhalant Effects
Inhalants are selected for misuse because of their “ability to rapidly induce euphoria,” as well as their stimulant, disinhibiting, and hallucinatory effects (Baydala et al., 2010, p. 443). As soon as these immediate effects diminish, the individual may experience depression, dizziness, disorientation, loss of coordination, slurred speech, drowsiness, and/or headache (Baydala et al., 2010). Specific to nitrite misuse is a drop in blood pressure (hypotension) that may lead to a loss of consciousness (syncope). Their misuse as a club drug is related to sexual effects (penile engorgement and sphincter relaxation conducive to anal sex; Baydala et al., 2010).
Inhalant misuse is extremely concerning as a public health issue because of the considerable potential for brain damage, damage to other organ systems, and lack of oxygen (hypoxia) associated with this form of substance misuse. Baydala et al (2010) report that sudden death may occur as a result of the physical effects of these chemicals (especially the heart); injury may result from engaging in risky behavior due to the disinhibiting effects these substances may have (drowning, falling, burns, or exposure to the elements/cold weather); and, suffocation (hypoxia, lack of oxygen) may occur in the process of using inhalants. In the long term, irreversible damage to the brain and other organ systems (heart, lungs, bone marrow, liver, kidneys) may result, especially (but not only) when chronic misuse occurs (Baydala et al., 2010).
Epidemiology of Inhalant Misuse
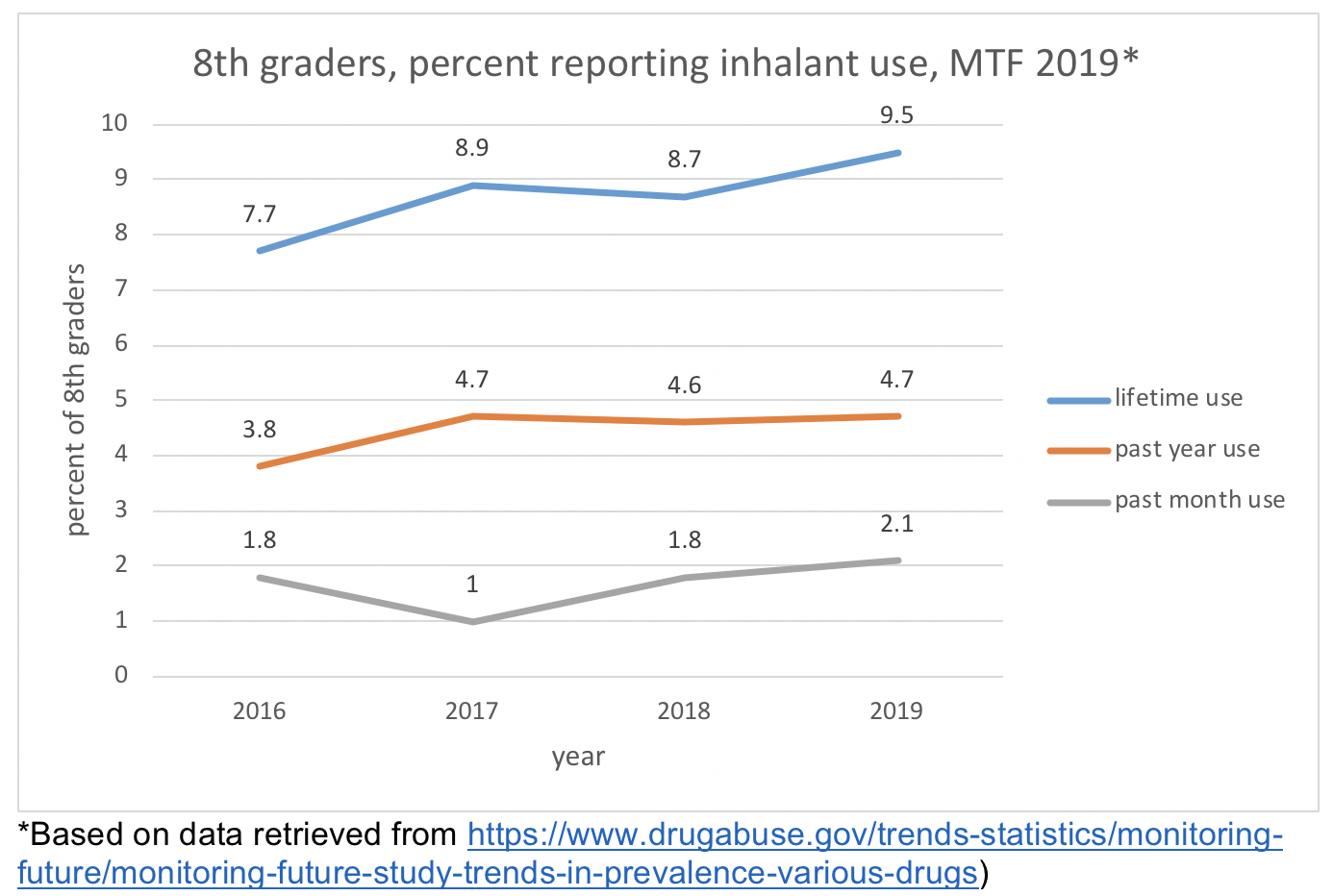
The 2019 Monitoring the Future (MTF; https://www.drugabuse.gov/trends-statistics/monitoring-future/monitoring-future-study-trends-in-prevalence-various-drugs) data show a perplexing trend in the comparison of 8th, 10th, and 12thgrade students’ report of lifetime inhalant use—the 8th grade cohort reported it more often than did 10th graders or 12th graders: 9.5% compared to 6.8% and 5.30%. With most other substances, lifetime use is greater as students age. (This 8th grade cohort also more often reported lifetime use of cough medicine misuse, heroin use, and methamphetamine use than did the 10th or 12th graders.) They also reported past year (4.70%) and past month (2.10%) inhalant misuse more often than their older peers (2.80% and 1.90% for past year misuse by 10th and 12thgraders; 1.10% and 0.90% for past month misuse by 10th and 12th graders). Data concerning a trend from 2016-2019 suggests that lifetime and past year inhalant misuse have increased significantly (see the trend chart below).
Inhalants are typically a “youthful” choice for substance misuse (NIDA, 2017a; Baydala et al., 2010). This point is reinforced by the 2019 NSDUH survey data (SAMHSA, 2019). In 2018, almost 25 million individuals (9.1% of the population) aged 12 and older in the U.S. were estimated to have engaged in inhalant misuse during their lifetime, over 2 million (0.7%) during the past year, and almost 700,000 (0.2%) during the past month. The past month (current) misuse of inhalants was reported by 0.7% of adolescents aged 12 to 17 years, 0.4% of emerging/young adults aged 18 to 25 years, and 0.1% of adults aged 26 or older.
 Lifetime reported inhalant use by individuals aged 12 and older was more common among men than women (11.8% versus 6.5%), however among the current cohort of 12 to17-year-olds, the statistics were almost equal with girls reporting at a slightly higher rate than boys (8.6% versus 8.5%). Within this same young cohort, lifetime inhalant use was most often reported by individuals self-identifying as being of two or more races (9.7%), White (9.2%) and Black or African American (8.7%). Unlike most of the other types of substances we have studied, Asian individuals in this young cohort were not the group with the lowest reported lifetime inhalant use (7.8%). This rate was similar to that reported by Hispanic or Latino individuals (8.0%) and greater than the rate reported by American Indian/Alaska Native individuals (5.1%). The 12 to 17-year-old cohort with lifetime inhalant use was estimated across the U.S. to be about 662,000 individuals.
Lifetime reported inhalant use by individuals aged 12 and older was more common among men than women (11.8% versus 6.5%), however among the current cohort of 12 to17-year-olds, the statistics were almost equal with girls reporting at a slightly higher rate than boys (8.6% versus 8.5%). Within this same young cohort, lifetime inhalant use was most often reported by individuals self-identifying as being of two or more races (9.7%), White (9.2%) and Black or African American (8.7%). Unlike most of the other types of substances we have studied, Asian individuals in this young cohort were not the group with the lowest reported lifetime inhalant use (7.8%). This rate was similar to that reported by Hispanic or Latino individuals (8.0%) and greater than the rate reported by American Indian/Alaska Native individuals (5.1%). The 12 to 17-year-old cohort with lifetime inhalant use was estimated across the U.S. to be about 662,000 individuals.
What is (Anabolic Androgenic) Steroid Misuse
Steroid misuse typically refers to the use of anabolic steroids in ways not medically prescribed. Anabolic (androgenic) steroids differ considerably from corticosteroid medications used for treating inflammation, such as occur in autoimmune disorders like rheumatoid arthritis, allergic reactions, eczema, or asthma events. Anabolic androgenic steroids (AAS) are synthetic compounds related to or mimicking testosterone, a hormone naturally occurring in the bodies of both men and women in differing amounts. Anabolic is the common name for these substances: anabolic refers to tissue building and androgenic means promoting masculine characteristics (DOJ, 2004). Medically, anabolic steroids may be used to address delayed puberty and loss of muscle mass with certain diseases (NIDA, 2018a).
Their misuse by athletes, body builders, and members of certain physically demanding occupations to boost strength and endurance, or recover from muscle injury, taps into the tendency to develop muscle with these compounds and typically involves doses 10 to 1000 times what is medically prescribed (NIDA, 2018a; WHO, 1993). Steroid misuse comes in multiple forms of administration: oral, injection, or topical application to the skin. Common names for anabolic steroids include roids, juice, pumpers, gym candy, arnolds, and weight trainers (DOJ, 2004). Various OTC health supplements introduce anabolic steroid precursor chemicals to the body, leading the body to produce more of the steroid than would normally occur—with some of the same effects as using steroids themselves (DOJ, 2004). The major source of illicit steroids is from other countries where prescriptions are not required (DOJ, 2004), raising the specter of poor quality and/or contaminated drugs (WHO, 1993).
Effects of (Anabolic) Steroid Misuse
In the short-term, steroid misuse does not have easily recognizable psychoactive effects. Compared to the other substances we have studied in this course:
“The most important difference is that steroids do not directly activate the reward system to cause a ‘high’; they also do not trigger rapid increases in the brain chemical dopamine, which reinforces most other types of drug taking behavior” (NIDA, 2018a).
The mental effects of steroid misuse are more likely to appear over time with repeated (and high dose) misuse. These include (NIDA, 2018a; WHO, 1993):
- paranoia, extreme jealousy, and delusions;
- impaired judgment;
- mania;
- extreme irritability and aggression (sometime called “roid rage”).
Other organ systems are also likely to be affected by steroid misuse, including the kidneys, liver, cardiac (heart enlargement, high blood pressure, increased risk of stroke or heart attack), and male sexual organs (testicular shrinkage, decreased sperm count/infertility, breast development, and increased risk for prostate cancer). In women, the effects tend to defeminize/masculinize the body (reduced breast size, loss of menstrual cycles, deeper voice, male-pattern baldness, growth of excess facial/body hair).
Steroids do have some degree of addictive potential (NIDA, 2018a) despite their differences from the other substances studied this semester. As a substance use disorder, it falls under the classification of “other substance-related disorder” in the DSM; the International Classification of Diseases (ICD-10) presents criteria for dependence specific to steroid misuse. These criteria include evidence of tolerance, withdrawal syndrome with reduced use, strong desire to take steroids, difficulty in controlling steroid use, and neglecting other interests and persisting in use despite harmful consequences. Steroid withdrawal symptoms include:
- steroid craving
- fatigue
- restlessness
- mood swings
- loss of appetite
- disordered sleep (insomnia)
- decreased sex drive
- depression (including suicidality).
Epidemiology of Steroid Misuse
According to the MTF 2019 data (https://www.drugabuse.gov/trends-statistics/monitoring-future/monitoring-future-study-trends-in-prevalence-various-drugs), lifetime, past year, and past month misuse by 12th graders is relatively uncommon (1.50%, 1.60%, and 1.60% respectively). Steroid misuse is considerably more common among men compared to women, being athletic is a significant predictor, and one study identified a considerable number of noncompetitive bodybuilders as being engaged in this practice (AlShareef & Marwaha, 2019). Multiple reports suggested that it is difficult to be much more precise about the epidemiology since so few substance-related studies ask about steroid use/misuse.

