Ch. 2: Other Hallucinogenic & Dissociative Substances
This chapter concerns hallucinogenic substances (hallucinogens) and includes several dissociative substances, as well. The chapter contents address both naturally occurring hallucinogens from the plant and animal world, and others that are synthesized. Because of enlightenment or spiritual associations, hallucinogens are among the oldest psychoactive substances known to be intentionally used by humans—possibly for as long as 10,000 years (Knox, 2016). Hallucinogenic trips (tripping) can be experienced as either enlightening, fascinating, wonderous or “bad,” fraught with creepiness, terror, distress, and anxiety—”bad” as in the flying monkeys from the Wizard of Oz movie, an alien popping out of your chest from the movie Alien, or a prolonged, inescapable, really bad dream.
The substances discussed in this chapter represent only a fraction of those used worldwide—many forms are used in relatively localized ways. An example of localized misuse comes from guides’ anecdotal accounts in Costa Rica who describe tourists becoming ill (or dying) from licking cane toads who produce poison for self-defense, but which contain hallucinogenic chemicals (bufotenine and possibly DMT), among other toxic chemicals. Toad-produced toxins may be fatal to natural predators (including dogs and crocodiles). Production of hallucinogenic products from close toad relatives in the southwest United States (Colorado River Toad) has led to these species becoming seriously endangered.

What are Hallucinogenic and Dissociative Substances
Hallucinogenic and dissociative substances are those known to distort a person’s perceptions of reality, altering a person’s thoughts, feelings, and awareness of their environment (mind-altering) to the point where sensations seem real although they are not (https://www.drugabuse.gov/publications/drugfacts/hallucinogens). Dissociative substances also alter a person’s sense of reality, inducing a sense of being disconnected or detached (dissociated) from reality and/or disconnected from control over one’s own body.
Hallucinogens, whether dissociative or not, are sometimes referred to as psychotomimetic—mimicking psychosis (Begun, 2020). Why, you might ask, would anyone want to mimic psychosis? The easier-to-answer question is “What are hallucinations like?” Sometimes the effect has been reasonably recreated in films as an altered state of consciousness. In some instances, past memories are re-experienced as current lived realities, seeming as real as when first experienced. This may be good, bad, or neutral quality memories—the problem being that a person cannot control or predict which will be experienced this way. Or, the experience can involve a sense of movement through space or time—flying, soaring, floating, being pulled along, or otherwise moving—when in reality, no such movement occurs. Someone might experience being in more than one place at the same time or becoming someone/something else: becoming a tree, being the ocean, or being inside the mind of your dog. Objects or people in the real world can take on strange shapes, colors, or sounds while things not present can be seen, felt, or heard. The experience may involve unreal sensations, including the sensory crossover: hearing colors or seeing sounds, for example. The kind of sensory crossover experience is called synesthesia.
In addition to their main psychoactive effects, many hallucinogenic substances also cause increased heart rate, blood pressure, and body temperature. They also may cause sleep disorder, and possibly paranoia or acute, severe panic. Hallucinogenic experiences may persist or recur well after the active ingredients have been fully metabolized and the drug’s effects have worn off (drug-related flashback). Dissociative substances also may cause numbness, amnesia, disorientation, inability to move, and trouble breathing, particularly when used on combination with other respiratory depressing substances. Anxiety and depression (including suicidal thoughts) associated with hallucinogen use may persist long-term after a period of regular use.
Examples of naturally occurring hallucinogenic substances are psilocybin (“magic mushrooms”), mescaline (peyote cactus), ayahuasca (DMT), and salvia divonorum (a plant in the mint family). Examples of synthesized hallucinogenic substances are LSD (lysergic acid diethylamide) and MDMA/ecstasy. Examples of synthesized hallucinogenic dissociative substances are PCP (phencyclidine), ketamine, and dextromethorphan (DXM), the substance in many cough medicines. You may also hear about synthetic products called bath salts (synthetic cathinones) which have both hallucinogenic and stimulant effects; these new psychoactive substances may temporarily skirt the law and DEA scheduling rules by rapidly changing their ingredients and being sold as plant food, jewelry cleaner, or phone screen cleaner, and labeled “not for human consumption” (NIDA, 2018a).
Let’s look at some of these substances in a little more detail, recognizing that according to the U.S. Drug Enforcement Agency (DEA), LSD, mushrooms, and ecstasy/MDMA are the most commonly misused hallucinogens (https://www.dea.gov/sites/default/files/sites/getsmartaboutdrugs.com/files/publications/DoA_2017Ed_Updated_6.16.17.pdf#page=84).

 DXM (dextromethorphan). DXM is a common ingredient in many cough suppressant medications. In high doses, DXM can induce hallucinogenic and dissociative effects. A complicating problem with high dose exposure to DXM in cough suppressant formulations is that the person is also ingesting exceedingly high doses of the other ingredients (antihistamines and decongestants) that can produce risky overdose effects themselves. Even at low doses DXM can cause distorted visual perceptions. Related to the name of one well-known manufacturer of cough medicines, Robo is a common nickname related to DXM misuse (NIDA, 2019b).
DXM (dextromethorphan). DXM is a common ingredient in many cough suppressant medications. In high doses, DXM can induce hallucinogenic and dissociative effects. A complicating problem with high dose exposure to DXM in cough suppressant formulations is that the person is also ingesting exceedingly high doses of the other ingredients (antihistamines and decongestants) that can produce risky overdose effects themselves. Even at low doses DXM can cause distorted visual perceptions. Related to the name of one well-known manufacturer of cough medicines, Robo is a common nickname related to DXM misuse (NIDA, 2019b).
Ketamine. Ketamine is another of the “club drugs” you read about in our module concerning sedative-hypnotic drugs. It was originally developed for anesthesia purposes and has some structural similarity to PCP (see below). It is briefly revisited here in our module concerning hallucinogenic and dissociative drugs because of its hallucinogenic effects and its effects on loss of body control and amnesia. Ketamine can create a dream-like state and/or altered perceptions. Flashback experiences have been reported with ketamine use. Other names used for ketamine include special K, K, super K, vitamin K, kit kat, keets, jet, purple, and cat valium. Acute effects include rapid heartrate, high blood pressure, and depressed breathing/apnea events, and use is associated with increased risk of injury because of its suppression of pain responses (Chakraborty, Neogi, & Basu, 2011). Ketamine is potentially addictive and chronic use may lead to reduced pain sensation, loss of coordination, difficulty with concentration, insomnia, drowsiness, slurred speech, and bladder incontinence. Withdrawal symptoms include loss of appetite, fatigue, irregular heartbeat, anxiety, depression, tremors, sweating, and chills, as well as nightmare disturbed sleep. Ketamine is often used in a mixed sequence of polydrug use involving stimulants (e.g., methamphetamine, cocaine) or heroin (Chakraborty, Neogi, & Basu, 2011). It is a Schedule III drug in the U.S. and currently the subject of some research into its potential in treating severe depression.
Kratom. Kratom powder, pills, and capsules are produced from the leaves of a tropical Asian plant with a mix of effects: at low doses kratom acts more as an energizing stimulant, while at higher doses acts more like an opioid, but can also have hallucinogenic effects. Thus, it is difficult to know where to classify kratom: often, it is listed in opioid discussions because of its pain-control actions. Kratom has potential use in opioid withdrawal but is considered a dangerous addictive substance itself (UNODC, 2012). Although some argue it is a safer alternative than certain prescription medications, its use has proven deadly in some cases. Kratom’s abuse potential and lack of evidence-based medical uses lead to its being declared an illicit substance in many countries and several of the United States. In 2016, the U.S. Drug Enforcement Agency (DEA) announced plans to declare kratom a Schedule I substance in the United States; however, intense public reaction contributed to the DEA’s reversal of this decision only 2 months later. As of 2017 kratom remains an unscheduled substance at the federal level but is listed as “a drug of concern” by the DEA.
 LSD (lysergic acid diethylamide). LSD is among the most powerful mind-altering substances in common use (NIDA, 2019b). Some common “street” names for LSD include acid, battery acid, blotter acid, boomers, California sunshine, sunshine, dots, microdot, doses, pane, windowpanes, sugar cubes, Lucy in the sky/Lucy, golden dragon, and mellow yellow—several of these nicknames refer to the ways that LSD is or has in the past been distributed (e.g., drops placed on sugar cubes or on scraps of blotter paper). LSD is synthesized from the product of a fungus known to grow on rye and some other cereal grains: ergot. Ergot-contaminated food/bread is attributed as the cause of historical community-wide mass hysterical/hallucination events; ergotamine is also an ingredient is several medications used to affect blood flow patterns related to migraine headaches and to induce uterine contractions (so it can also cause miscarriage).
LSD (lysergic acid diethylamide). LSD is among the most powerful mind-altering substances in common use (NIDA, 2019b). Some common “street” names for LSD include acid, battery acid, blotter acid, boomers, California sunshine, sunshine, dots, microdot, doses, pane, windowpanes, sugar cubes, Lucy in the sky/Lucy, golden dragon, and mellow yellow—several of these nicknames refer to the ways that LSD is or has in the past been distributed (e.g., drops placed on sugar cubes or on scraps of blotter paper). LSD is synthesized from the product of a fungus known to grow on rye and some other cereal grains: ergot. Ergot-contaminated food/bread is attributed as the cause of historical community-wide mass hysterical/hallucination events; ergotamine is also an ingredient is several medications used to affect blood flow patterns related to migraine headaches and to induce uterine contractions (so it can also cause miscarriage).
 MDMA/ecstasy. MDMA, commonly called ecstasy (sometimes XTC) or Molly, is a hallucinogen with stimulant effects. The psychoactive effects of MDMA involve increased activity among three neurotransmitters (NIDA, 2018b): dopamine (reward system reinforcing behavior), norepinephrine, and serotonin (mood, appetite, sleep, sexual arousal, pain sensation). MDMA use can cause dangerously high body temperature, elevated blood pressure, and rapid heart rate, especially when a person’s increased energy leads to high levels of physical activity. MDMA/ecstasy is often addressed as a “club drug” but its use is not limited to those environments. It is listed as a Schedule I drug by the U.S. DEA; because distribution is illegal, what MDMA an individual acquires to use may be heavily contaminated with toxic chemicals or other drugs. MDMA appears to have an addictive potential, although the evidence is unclear (NIDA, 2018); “almost 60% of people who use ecstasy report withdrawal symptoms” and as many as 43% have met three or more criteria for substance use disorder related to this drug (https://www.drugs.com/illicit/ecstasy.html). Confusion, depression, anxiety, sleep disorders, and craving are known effects of either MDMA use or withdrawal, and in nonhuman primates MDMA has proven to be toxic to neurons in the mood, thinking, and judgment areas of the brain—just 4 days of MDMA exposure caused damage that remained evident years later (https://www.drugs.com/illicit/ecstasy.html).
MDMA/ecstasy. MDMA, commonly called ecstasy (sometimes XTC) or Molly, is a hallucinogen with stimulant effects. The psychoactive effects of MDMA involve increased activity among three neurotransmitters (NIDA, 2018b): dopamine (reward system reinforcing behavior), norepinephrine, and serotonin (mood, appetite, sleep, sexual arousal, pain sensation). MDMA use can cause dangerously high body temperature, elevated blood pressure, and rapid heart rate, especially when a person’s increased energy leads to high levels of physical activity. MDMA/ecstasy is often addressed as a “club drug” but its use is not limited to those environments. It is listed as a Schedule I drug by the U.S. DEA; because distribution is illegal, what MDMA an individual acquires to use may be heavily contaminated with toxic chemicals or other drugs. MDMA appears to have an addictive potential, although the evidence is unclear (NIDA, 2018); “almost 60% of people who use ecstasy report withdrawal symptoms” and as many as 43% have met three or more criteria for substance use disorder related to this drug (https://www.drugs.com/illicit/ecstasy.html). Confusion, depression, anxiety, sleep disorders, and craving are known effects of either MDMA use or withdrawal, and in nonhuman primates MDMA has proven to be toxic to neurons in the mood, thinking, and judgment areas of the brain—just 4 days of MDMA exposure caused damage that remained evident years later (https://www.drugs.com/illicit/ecstasy.html).
 Mescaline (peyote). While mescaline is naturally occurring in peyote cactus buds (buttons or mescal buttons) and a few other plant types, it can also be synthetically produced (NIDA, 2019b). Generally illegal to possess in the U.S., some religious ceremony uses by Native Americans is allowed. Mescaline causes “rich visual hallucinations” (https://www.drugs.com/illicit/mescaline.html), similar to those experienced with LSD or psilocybin (see below). Use also may be accompanied by a distorted (slowed) sense of time and synesthesia (seeing sounds, hearing colors). Its use may be accompanied by a racing heart rate, acute anxiety, headache, accidental injury, amnesia, vomiting, or seizures (https://www.drugs.com/illicit/mescaline.html). Although not considered to be addictive, individuals may develop tolerance, requiring increasing amounts to achieve the same effects—which also increases the potential for negative side effects.
Mescaline (peyote). While mescaline is naturally occurring in peyote cactus buds (buttons or mescal buttons) and a few other plant types, it can also be synthetically produced (NIDA, 2019b). Generally illegal to possess in the U.S., some religious ceremony uses by Native Americans is allowed. Mescaline causes “rich visual hallucinations” (https://www.drugs.com/illicit/mescaline.html), similar to those experienced with LSD or psilocybin (see below). Use also may be accompanied by a distorted (slowed) sense of time and synesthesia (seeing sounds, hearing colors). Its use may be accompanied by a racing heart rate, acute anxiety, headache, accidental injury, amnesia, vomiting, or seizures (https://www.drugs.com/illicit/mescaline.html). Although not considered to be addictive, individuals may develop tolerance, requiring increasing amounts to achieve the same effects—which also increases the potential for negative side effects.
PCP (phencyclidine). PCP is classified as a dissociative substance with hallucinogenic effects. Common “street” names include angel dust, wack, ozone, dust, peace pills, embalming fluid, rocket fuel; cannabis is laced with PCP may be called supergrass, superweed, whacko tobacco, or killer joints (https://www.drugs.com/illicit/pcp.html). PCP interacts with an array of neurotransmitter sites (including NMDA, glutamate, dopamine, opioid, and nicotinic receptors). Auditory hallucinations may accompany visual distortions with PCP use. Individuals may experience acute anxiety or paranoia which may contribute to them erupting into hostile violence; some individuals experience an overwhelming sense of dread or impending doom which may contribute to attempted suicide (https://www.drugs.com/illicit/pcp.html). PCP is potentially addictive and long-term use may lead to memory loss, cognitive/learning difficulties, depression, and significant weight loss. Because PCP interacts with alcohol and other CNS depressants (e.g., benzodiazepines), overdose risk is increased when these substances are combined.
 Psilocybin. Multiple species of fungi (mushrooms) contain the active ingredient psilocybin and/or psilocin, hence they are often called psychedelic or magic mushrooms, they may also be referred to as mushies, sacred mushrooms, or zoomers. Because of the potential for abuse and the absence of evidence-based medical uses, psilocybin is a Schedule I substance in the United States (and many other United Nations countries). However, in recent years increasing scientific interest has been directed toward the potential for psilocybin to treat various physical and mental conditions, including intense cluster headaches, depression, and extreme anxiety. Should these studies result in strong supporting evidence, it is possible that the DEA could revise the schedule level for this substance. One problem with psilocybin mushrooms is that they closely resemble other types that are poisonous. Another problem is that their potency varies dramatically by mushroom species, growing conditions, and how they are handled/time since harvesting. For example, the concentration in dried mushrooms is considerably higher than in their fresh counterparts (https://www.medicalnewstoday.com/articles/308850.php#what-is-psilocybin). Although psilocybin is considered non-addictive, individuals may develop tolerance with regular use and possibly cross-tolerance to other hallucinogenic substances (e.g., LSD and mescaline; https://www.medicalnewstoday.com/articles/308850.php#abuse-potential).
Psilocybin. Multiple species of fungi (mushrooms) contain the active ingredient psilocybin and/or psilocin, hence they are often called psychedelic or magic mushrooms, they may also be referred to as mushies, sacred mushrooms, or zoomers. Because of the potential for abuse and the absence of evidence-based medical uses, psilocybin is a Schedule I substance in the United States (and many other United Nations countries). However, in recent years increasing scientific interest has been directed toward the potential for psilocybin to treat various physical and mental conditions, including intense cluster headaches, depression, and extreme anxiety. Should these studies result in strong supporting evidence, it is possible that the DEA could revise the schedule level for this substance. One problem with psilocybin mushrooms is that they closely resemble other types that are poisonous. Another problem is that their potency varies dramatically by mushroom species, growing conditions, and how they are handled/time since harvesting. For example, the concentration in dried mushrooms is considerably higher than in their fresh counterparts (https://www.medicalnewstoday.com/articles/308850.php#what-is-psilocybin). Although psilocybin is considered non-addictive, individuals may develop tolerance with regular use and possibly cross-tolerance to other hallucinogenic substances (e.g., LSD and mescaline; https://www.medicalnewstoday.com/articles/308850.php#abuse-potential).
Salvia divornum. Salvia divornum’s original use among indigenous groups in Mexico involved ritual divination in spiritual contexts. The plant’s leaves can be chewed or smoked and the active ingredient, salvinorin A, induces visual hallucinogenic effects, as well as distorted bodily sensations and movement. Salvia divornum is currently unscheduled by the U.S. DEA but is illegal in some states.
Epidemiology of Hallucinogenic Use
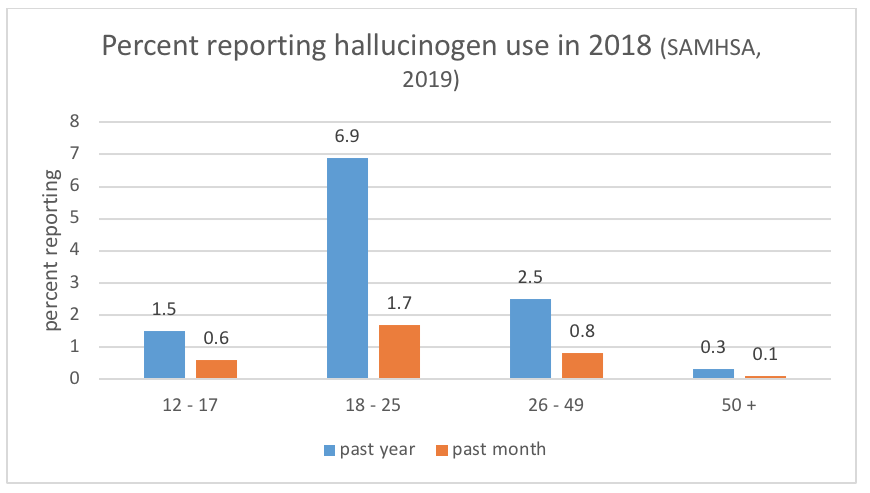
Based on data from the 2018 National Survey on Drug Use and Health (NSDUH, SAMHSA, 2019) we can see once again that the age group most commonly reporting the use of these substances were emerging adults, 18 to 25-year-olds. However, compared to many other substances (e.g., alcohol, cannabis, stimulants, sedatives, opioids) the rate of hallucinogenic use is considerably lower.
The rate of overdose deaths from hallucinogens is described by the DEA as “extremely rare” https://www.dea.gov/sites/default/files/sites/getsmartaboutdrugs.com/files/publications/DoA_2017Ed_Updated_6.16.17.pdf#page=84.However, the DEA reports that deaths related to their use do occur—typically from accidents, engaging in risky/dangerous behaviors, toxicity or poisoning by contaminants, and suicide.
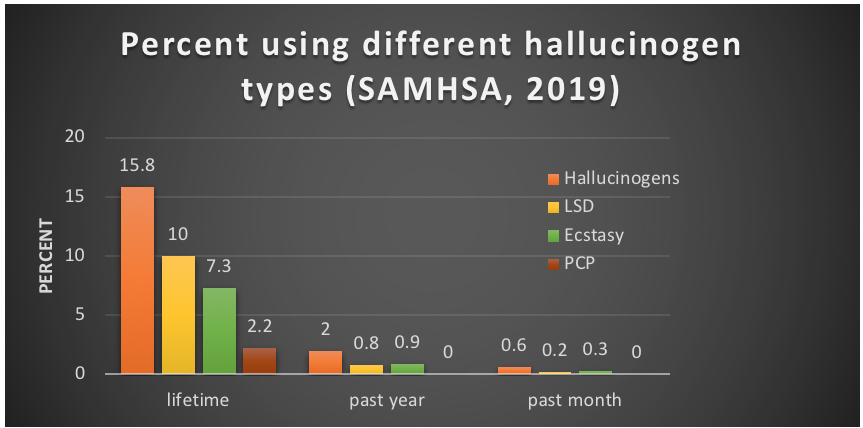
The 2018 NSDUH data (SAMHSA, 2019) can help develop an understanding of which hallucinogenic substances are used most often in the U.S. by individuals aged 12 and older. The results for lifetime, past year, and past month use of hallucinogens in general, LSD, PCP, and ecstasy are presented in the following graph. As you can see, LSD was the most commonly reported of the hallucinogens and PCP the least.

STOP & THINK
Turn on the iTunes visualizer to display animations of some favorite songs or visit the following YouTube sites to experience how sensory crossover might be experienced—visualizations of music/sound.
Consider what might it be like for someone to live a unique visual/auditory experience through use of hallucinogens. Then consider what might be like if they were to encounter an anxiety producing visual/auditory experience instead?
Consider what you have been learning about hallucinogenic substance misuse: how would you advise someone who was considering using LSD, peyote, or mescaline for the first time?
